

Share this
on July 16, 2019
Most dental implants patients are usually older adults who have lost some or all dentition over the course of many years. On the other hand, corrective jaw surgery patients tend to be younger, those in their late teens and twenties. However, there is a group of patients who have dentofacial deformities that require orthognathic surgery but somehow did not get around to doing it when they were younger but in their later years, require dental implants to replace their missing or failing dentition. For such patients, orthognathic surgery may be done in conjunction with dental implants to restore not just a functional dentition but an improvement of facial aesthetics as well.
In the Singapore context, the underbite, where the lower jaw is disproportionately longer than the upper jaw, is the least accepted dentofacial deformity and hence the most commonly corrected with surgery. Other deformities seem to be better tolerated. Deformities such as an overbite, where the lower jaw is significantly shorter that the upper jaw, and bimaxillary protrusion, where both the upper and lower jaws are disproportionately longer than the skull base, are often left uncorrected surgically.
When patients with such skeletal deformities age and lose teeth, a second opportunity to correct such deformity presents itself. I will illustrate what can be done in such cases using the following example.
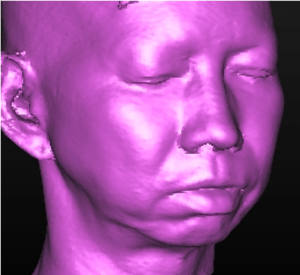 A middle-aged lady with bimaxillary protrusion, short lower jaw, missing upper front teeth and missing lower molars and the remaining teeth with decay and gum disease. This lady would like to have her short lower jaw lengthened and a full mouth rehabilitation including replacement of missing teeth with dental implants.
A middle-aged lady with bimaxillary protrusion, short lower jaw, missing upper front teeth and missing lower molars and the remaining teeth with decay and gum disease. This lady would like to have her short lower jaw lengthened and a full mouth rehabilitation including replacement of missing teeth with dental implants.
What are the treatment options?
In a situation where both facial aesthetics and dental function are involved, I always plan the facial aesthetics first. Facial aesthetics takes priority because the dentition and occlusion can be restored aesthetically and functionally within an aesthetically proportioned face. However, a dentofacial deformity cannot be corrected without changing the pre-existing teeth alignment. If the teeth were restored first, any subsequent surgery to correct the dentofacial deformity will require a complete change of the dental restorations.
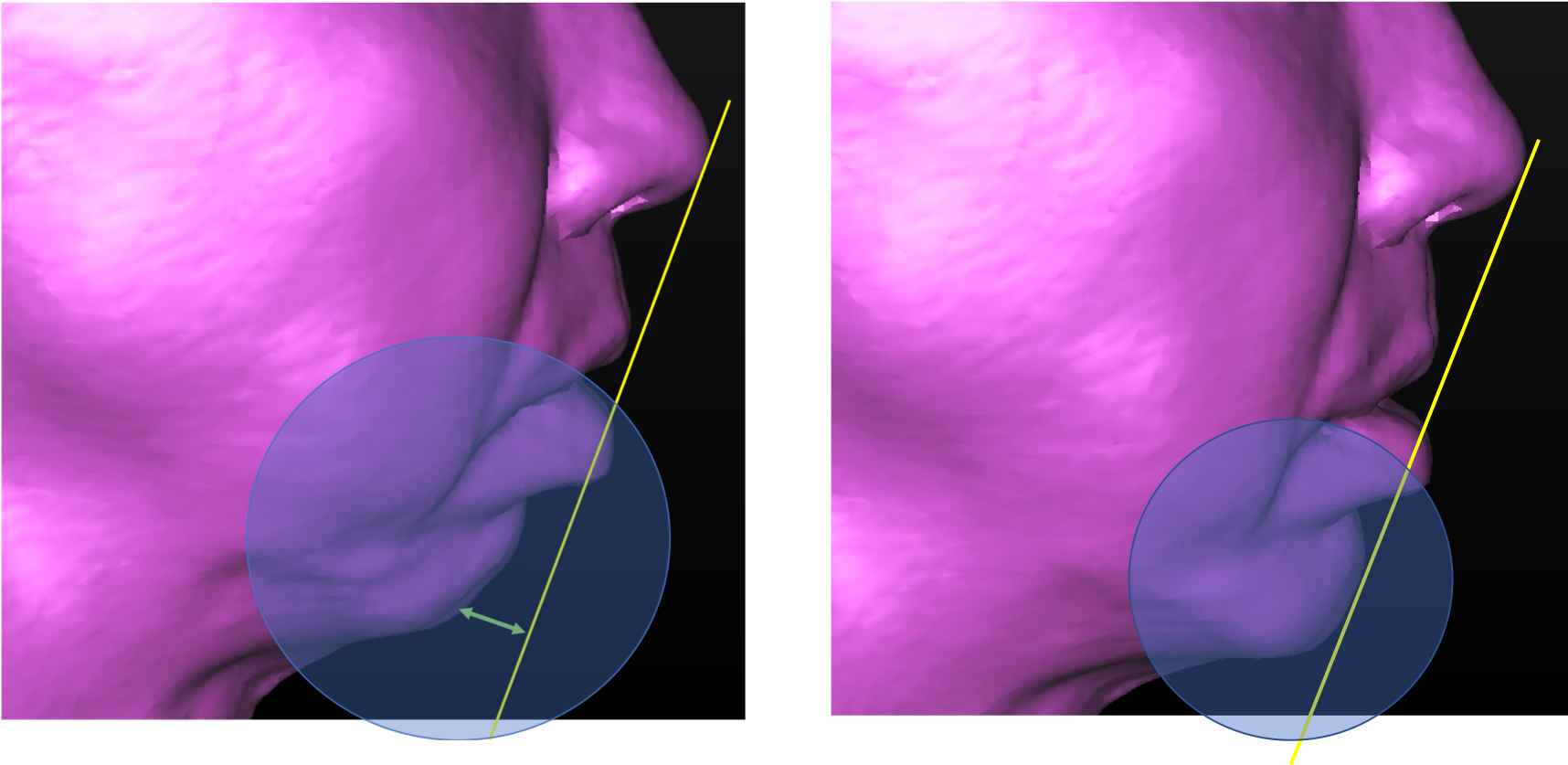
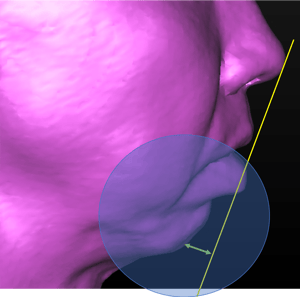 Looking at the facial proportions, the lower jaw is significantly deficient. The chin point is located close to the throat, giving the appearance of a non-existent chin. However, while the lower jaw is short, the teeth are protruding forward excessively. This excessive forward development of the lower front teeth causes the lips to be incompetent, i.e. unable to meet the upper lip passively without contracting the muscles around the lips.
Looking at the facial proportions, the lower jaw is significantly deficient. The chin point is located close to the throat, giving the appearance of a non-existent chin. However, while the lower jaw is short, the teeth are protruding forward excessively. This excessive forward development of the lower front teeth causes the lips to be incompetent, i.e. unable to meet the upper lip passively without contracting the muscles around the lips.
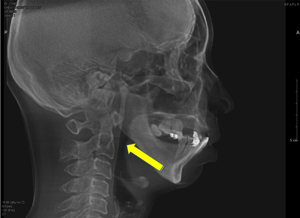 The small lower jaw also poses a risk of obstructive sleep apnea, a sleep disorder whereby the airway is obstructed during sleep, causing prolonged periods where the body lacks oxygen.
The small lower jaw also poses a risk of obstructive sleep apnea, a sleep disorder whereby the airway is obstructed during sleep, causing prolonged periods where the body lacks oxygen.

 The upper jaw has lost all the front teeth and the bone has receded. Otherwise, the front teeth will also be protruding. With the loss of the teeth and the shrinkage of the bone, the upper jaw proportion has “self-corrected”.
The upper jaw has lost all the front teeth and the bone has receded. Otherwise, the front teeth will also be protruding. With the loss of the teeth and the shrinkage of the bone, the upper jaw proportion has “self-corrected”.
Looking inside the mouth, the teeth were found to be in bad shape. There is generalized gum disease and many teeth were decayed or infected. In the upper jaw, the back teeth are still present while the front teeth are missing. In the lower jaw, however, it is the opposite, the front teeth are present and the back teeth are missing.
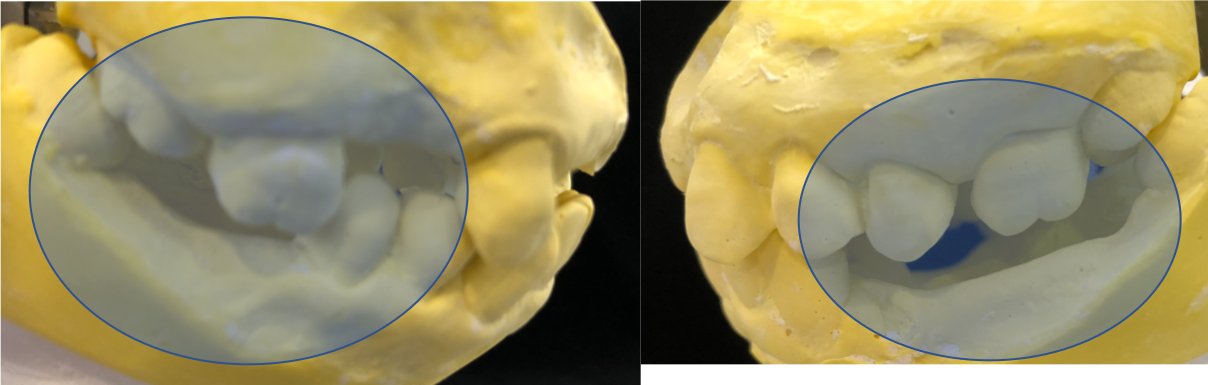
This combination results in a poor masticatory function as there are no opposing teeth for proper biting of food. It has also resulted in “super-eruption” of the teeth due to a lack of contact against opposing teeth. The upper back teeth have migrated downwards towards the lower jaw and the lower front teeth have migrated upwards toward the upper jaw.
Overall, this patient has a small lower jaw which poses an aesthetic challenge as well as potential for obstructive sleep apnea. The teeth require extensive restorative work if they were to be saved. Bearing in mind the patient’s objective of improving her appearance and bite, several options are available.
First, an ambulatory sleep study can be done to screen for obstructive sleep apnea. Depending on the results of the study, options for treatment will be discussed. If the obstruction was found to be due to the small lower jaw, treatment of the OSA will coincide nicely with the overall facial aesthetic surgery as well as the restorative dentistry.
To improve facial aesthetic, the lower jaw will need to be lengthened. If surgery is done to lengthen the lower jaw alone, it will further exacerbate the protruding teeth. As such, any surgery to lengthen the base of the lower jaw will need to be accompanied by a surgery to set the front teeth backwards as a block followed by orthodontic alignment. However, in this particular case, the front teeth are not in a good state. Some are decayed, others have gum disease. As such, given the guarded long-term survival of the teeth, an alternative is to extract them and replace with dental implants instead of surgically repositioning them.
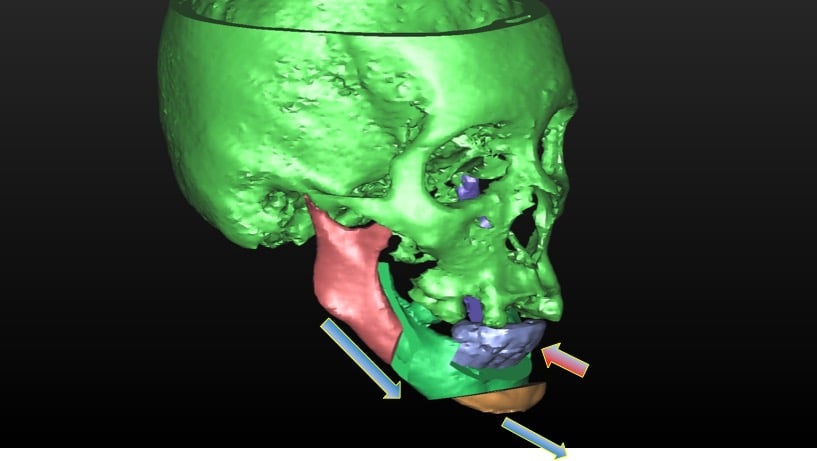
In addition to lengthening the lower jaw, the chin needs to be surgically repositioned into a more forward position. This additional procedure serves two purposes. Increasing the chin projection reduces the degree of lip incompetence and improves the aesthetic outcome. In addition, it also pulls the tongue muscles forward, further opening up the airway and hence reducing the risk of obstructive sleep apnea.
From the facial aesthetic perspective, the upper jaw does not need repositioning. However, as the back teeth has erupted excessively downwards, the back part of the upper jaw needs to be surgically repositioned upwards to re-establish a level set of teeth. Alternatively, the teeth can be extracted and replaced with dental implants.
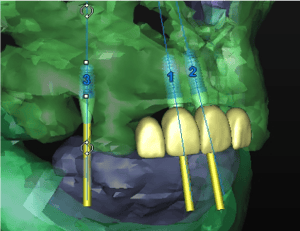
Dental implants require sufficient bone mass for insertion. There is insufficient bone in the upper jaw for implants and as such, the bone needs to be augmented. This is done as a bone grafting procedure, whereby bone from the hip is harvested and transferred to the upper jaw. In parts of the jaw where there is sufficient bone for initial stable fixation of the implant, the implant and bone graft can be done simultaneously. Otherwise, the bone graft is allowed to consolidate and integrate with the recipient site for six months before the implants are placed.
While the treatment objective is clear, there are many different paths to achieving those objectives. Each option has its pros and cons. A complex case like this often requires several sessions of discussion to ensure a common understanding of what the goals are and what the limitations of each options are. An ideal plan is one that is suited to what the patient values. Restoring all the teeth and orthodontically aligning them in conjunction of with orthognathic surgery may be ideal for one patient but extracting all the teeth and replacing them with dental implants may be preferred by another. There are cost and time considerations which are unique to each individual.

Share this
Subscribe by email
Email subscription

Comments (3)